

Back to Back Blog

Why Strength Training Is Essential for Injury Protection in the London Marathon
Training for the London Marathon is a huge physical undertaking. Over 26.2 miles, your body absorbs thousands of repetitive loading cycles. Every step places forces of two to three times bodyweight through your feet, ankles, knees and hips. Multiply that by 35,000–45,000 steps and it’s easy to see why injury rates in marathon training are high.
The common misconception? That more running is always the answer.
In reality, strength training is one of the most effective tools we have for injury protection in marathon runners. At our clinic in SW18, we regularly see runners who could have avoided weeks off training with a smarter strength foundation.
Here’s why it matters — and what to focus on.
The Marathon Is a Muscular Endurance Event
Marathon training is not just cardiovascular — it is muscular endurance under fatigue.
As fatigue builds:
Stride length shortens
Cadence drops
Hip control reduces
Ground contact time increases
This alters load distribution through the lower limb. When tissues fatigue, joints absorb more force. That’s when problems start.
Common marathon injuries include:
Achilles tendinopathy
Plantar fascia irritation
Patellofemoral knee pain
IT band pain
Bone stress injuries
In many cases, the root cause is not “tightness” — it’s insufficient strength and tissue capacity for the demands placed upon them.
Strength Improves Tissue Capacity
Every tendon, muscle and bone has a load tolerance threshold. Training increases that threshold.
When you perform progressive strength training:
Tendons become stiffer and more resilient
Muscles generate force more efficiently
Bones respond to loading by strengthening
Neuromuscular control improves
This creates what we call load capacity — the ability to tolerate marathon training without breaking down.
Without this, your running volume can outpace your body’s ability to adapt.
The Calf Complex: The Unsung Hero
The calf complex (gastrocnemius and soleus) is one of the most overloaded structures in marathon running.
The soleus, in particular, works tirelessly to control forward momentum and absorb force during stance phase. As fatigue builds late in the race, reduced calf capacity often leads to:
Achilles overload
Plantar fascia strain
Shin pain
Specific strength work should include:
Straight-leg calf raises (gastrocnemius bias)
Bent-knee calf raises (soleus bias)
Heavy, slow resistance work
High-repetition endurance sets
Many runners underestimate how strong their calves need to be for 26.2 miles.
Hip Strength Protects the Knee (your knee IS your hip!!!)
Poor hip strength and control can increase load through the knee and IT band.
When the gluteal muscles fatigue:
The knee drifts inward
Femoral rotation increases
Patellofemoral stress rises
Over thousands of strides, this becomes painful.
Key exercises include:
Single-leg deadlifts
Split squats
Step-downs
Lateral band walks
Side planks
The goal is not bodybuilding. It is controlled, unilateral strength under load.
Strength Reduces Fatigue-Related Breakdown
Research consistently shows that strength training:
Improves running economy
Reduces ground contact time
Enhances force production
Better economy means less energy cost per stride. That translates to reduced fatigue late in the race — and fewer compensatory movement patterns.
Injury risk increases significantly in the final third of marathon training blocks, when mileage peaks and cumulative fatigue is highest. Runners who maintain strength work during this phase tend to cope better.
“But I Don’t Want to Be Too Sore to Run”
A common concern.
The solution is intelligent programming:
Two sessions per week
30–40 minutes
Focus on lower limb and trunk
Avoid excessive new exercises during peak mileage
Reduce volume slightly in taper phase
Strength training should complement running, not compromise it.
Heavy lifting during base phase. Maintenance during peak weeks. Light activation during taper.
Bone Health and Stress Fracture Protection
Bone responds positively to load — but it needs varied stimulus.
Running is repetitive. Strength training introduces different loading patterns that stimulate bone adaptation.
This is especially important for:
Female athletes
Masters runners
Runners increasing mileage
Those with a history of bone stress injury
Under-fuelling combined with high mileage and no strength training is a high-risk scenario.
Practical Weekly Structure (just some ideas…)
A simple template might look like:
Day 1: Lower Limb Strength
Split squats
Romanian deadlifts
Straight-leg calf raises
Core control
Day 2: Stability and Endurance
Step-downs
Bent-knee calf raises
Single-leg bridges
Side planks
Keep it progressive. Add load when movements feel controlled and technically sound.
Strength Training Is Performance Training
This isn’t just about avoiding injury.
Stronger runners:
Maintain pace longer
Resist form breakdown
Produce more force per stride
Feel more robust during peak training
The London Marathon rewards durability.
Final Thoughts
Marathon training already places huge demand on the body. Relying on running alone is often not enough to prepare tissues for the cumulative load of 26.2 miles.
Strength training:
Increases tissue capacity
Reduces fatigue-related movement breakdown
Protects against common overuse injuries
Improves performance
If you’re building towards the London Marathon, investing in strength now could be the difference between standing on the start line — or sitting out injured.
Run consistently. Lift intelligently. Arrive strong.
For more advice book into see one of our osteopaths at the clinic in Wandsworth SW18.
Look at our blog on bone stress injuries here
By James Dodd BSc (hons) Ost. FAFS.
GOsC registered

Hypermobility Spectrum Disorder and Ehlers-Danlos Syndrome
Hypermobility is often a general term given to those whose bodies are able to move and stretch more than is considered for the normal range of motion. In this blog I will mainly talk about the musculoskeletal (MsK) presentations of this disorder. You can get this at a local joint level or more generalised global joint level. Further reading can be from the EDS society.

Hypermobility is often a general term given to those whose bodies are able to move and stretch more than is considered for the normal range of motion. In this blog I will mainly talk about the musculoskeletal (MsK) presentations of this disorder. You can get this at a local joint level or more generalised global joint level. Further reading can be from the EDS society.
Over the years in the UK, specialists like Rodney Grahame started to make the suggestion that for some, being hypermobile, could be a problem. He and his team noted there seemed to be a link between flexible or very flexible people and pain. He felt that it was often overlooked and that so much of the time these patients were being misdiagnosed and so mismanaged.
In the earlier days of diagnoses, Hypermobility Syndrome (HMS) was the name given to patients whose joints moved outside their normal range and also had pain. Diagnostic criteria such as the Beighton and Brighton scores were used. HMS was also called Hypermobility Type 3, which was part of the larger syndrome of connective tissue disorders called Ehlers-Danlos Syndrome or EDS.
Over time and with increased awareness, further understanding and renewed research, the original diagnostic thoughts are still used, with the additional of new criteria. The diagnosis given to patients has also changed and been broken down to more specific Hypermobility Spectrum Disorder (HDS) or Hypermobile EDS (hEDS). There are differences to each of these…
The main differences between HDS and hEDS are beyond the need for this paper and the differences need to be thoroughly looked at by a doctor/osteopath/physiotherapist/chiropractor with an interest in this area before a complete diagnosis is given. Having the correct diagnosis and treatment plan is more important that giving patients labels.
In a nutshell, and from a MsK point of view, both HSD and hEDS can make tissues more vulnerable to overstrain and injury. It can be painful, extremely frustrating and lead to fear and anxiety. I also think it is important to add here that pain is so much more complex than we used to think and it is not just a measure of increased pain equals more tissue damage.
Diagnosis
The diagnosis of HDS/EDS needs to be from a medical doctor or a qualified practitioner such as a registered osteopath, physiotherapist or chiropractor with a specialist interest.
A thorough case history, family history and examination needs to be completed to get a full understanding as to why the patient is suffering and to make a comprehensive diagnosis. The list of signs and symptoms linked to HSD/hEDS can be extensive.
A look at the conditions
For some with HSD or hEDS the symptoms could be at all levels of the spectrum from the very mild to more severe and/or all levels in-between.
A list of signs and symptoms could be long and could be widespread, but it covers chronic muscle, tendon, ligament or joint pain. This pain is often (although not always) relieved by rest. Ankles that sprain easily, clicky joints, a jaw that clicks. It may have been an incident (such as an ankle sprain) that his triggered a set of symptoms. Patients with HDS/hEDS are often clumsy, may get foggy thought patterns and fatigue more easily that others. Other symptoms that can coexist are palpitations, abomination concerns, anxiety, POTS (postural orthostatic tactical syndrome) or mast cell activation syndrome (MCAS).
Osteopathic TT for treatment for the severe HSD/hEDS patient ideally needs a team of like minded practitioners that address the needs of the patient.
From my point of view, Msk treatments need to be aimed at giving some pain relief and giving the patient strategies to manage their pain and movement patterns. I tend to avoid giving patients stretching to do as I feel that this could lead to more instability going forwards. This can lead to more chronic muscle tightness and pain as the body tries to protect itself by creating more tightness to stabilise itself.
I feel that osteopathy is great at providing relief for pain using gentle treatments and manipulation and some acupuncture. The more this is layered in with a gradual and progressive exercise programme to increase the patients capacity the better.
HDS/hEDS patients are a tough population to work with as there can be many bumps in the road of the journey. Just as they feel better, something else can start to become aggrieved. So, it is for this reason, that I feel that education for the patients is so key. For them to understand that pain is not always dangerous, it is just a message that is important. They need to be treated as a whole. They also need to also be aware of how vulnerable their bodies can be to changes that try to occur over and above the rate at which their body can adapt. Bodies can and do adapt. Those with HSD or hEDS can take longer to gain more capacity and resilience.
As our bodies gain greater capacity, they are able to deal with more. That is what strength and control is all about. Stretching does not give you greater ability to lift things in the garden or to bend to lift your child off the floor. Strength does!

From a movement point of view, aiming for efficiency and balance is useful so that one part of ones body is not talking all the hit for something else that is not working. Gait assessment can be useful to see what part of the patients gait makes the rest of their system struggle.
I often use the expression that I want people to have ‘reactive bodes’. What I mean by this is your bodies move and your muscles react to the movement. This sort of goes away from the ‘bracing’ model (unless you are picking 100kgs off the floor!!), which I am not sure I agree with.
By bracing or ‘pre-tensioning’ our body, it does not allow our body to move as it should and it isolates certain areas. Our bodies are amazingly integrated. When we move, no muscle EVER works by itself and so I am not sure how useful it is to isolate muscles when we exercise.
If you use a ‘Clam’ exercise as an example. This is when we lie on our side and lift the top leg up and down to ‘isolate’ and work your gluteus medius muscle. First of all, this muscle NEVER, ever works by itself when we move. But also, depending on your size and weight, the weight of your leg is not even close to what is needed to walk, run and squat etc. This muscle works as part of a ‘team’ of muscles and so are all best served working together as this is what happens when we move.
Having HDS/hEDS can certainly put challenges in front of you. There can be a few or many bumps along the road. But it does not mean that you cannot have a full life. As with many medical problems having a good mindset, a thorough understanding and having good capacity in your body all just helps. It is also ok to be frustrated with your body at times. Having a great bunch of people around you too massively helps.
Blog post by James Dodd BSc (hons) Ost. FAFS. Registered with the GOsC

The importance of sleep and a good mattress
Those that know me, know that I think the top 3 things (other than the building you live in) that you should spend money on is a great bed, amazing shoes and eyewear - gotta look after those eyes!. All are important things for our comfort and health. Have you ever acknowledged how you feel if your feet are uncomfortable or you sleep quality is poor? Your stress levels go up! A wonderful bed ideally should come high on your list.

Sleep ?
What is good sleep?
“a condition of body and mind that typically occurs for several hours every night, in which the nervous system is relatively inactive, the eyes closed, the postural muscles relaxed, and consciousness is practically suspended”.
As far as I am concerned, sleep is supposed to be a wonderful experience in a place where your body is able to relax and your ‘contours’ are looked after and supported. A great bed ‘has got you!’
Those that know me, know that I think the top 3 things (other than the building you live in) that you should spend money on is a great bed, amazing shoes and eyewear - gotta look after those eyes!. All are important things for our comfort and health. Have you ever acknowledged how you feel if your feet are uncomfortable or you sleep quality is poor? Your stress levels go up! A wonderful bed ideally should come high on your list.
There are many sleep statistics, but on average, the average person spends around 26 years of THEIR life sleeping. That is about a third of our lives!! Flip……!! And ……the average person also spends 7 years trying to drop off to sleep!!! Yikes. A major factor that will determine how well you sleep will be your comfort. If you are unable to get comfortable in your bed, the quality of your sleep will be poor and you may wake throughout the night. This doesn’t adhere to the definition of consciousness suspended. YOU know when you don’t sleep well.
Many patients we see at the clinic have mattresses that are VERY old, and many will just be unsupportive and sagging in the wrong places. An old mattress will also not be hygienic.
January sales will be upon us very soon. They may even start before Christmas!! Mattresses and beds can have various offers throughout the year… not just in January. So if you look at your bed and feel that it is actually about time to change it, be armed with as much information as you can be to make your purchase a success. It is also good to be aware of the return policies and T&Cs if you get your new purchase home and you are not happy. Some companies will only offer an exchange rather than return your money. So beware.
I actually think it is pretty tough to tell anyone what bed would be right for them for many reasons. They may have a partner of different size and weight. The may run ‘hot’ at night and so need a bed with more ventilation. They may have pets sleeping with them or children who join them at night. They may just just prefer a harder of softer bed. Ideally, I think you should be able to try the bed/mattress before you take the plunge. If you do buy online, make sure you can get a full refund if you don’t like it. And that you are not slapped with high costs if you need to return it.
‘Which?’ magazine has recently done another one of their great ‘test labs’ for mattresses. These reviews have been a great resource for many for nearly 50 years and they put each mattress tested through a battery of tests, looking at body support including how well it will look after you in each of the different ways many of us sleep. They test the durability of each one and they don’t just look at the expensive mattresses. What a great resource!!!
I am unable to give you all of their results. But the ones that come top of their reviews are:
Eve - The Original Hybrid
Emma-Premium
Emma - Start Hybrid
Memory Foam Warehouse - Coolmax Hybrid
Otty - Hybrid Mattress
And even Ikea Hamarvik came 6th in the list.
Interestingly , they do have a few VERY expensive ones in their tests and while they are good mattresses, they do not score near the top of their reviews.
Note that ALL of them (other than Ikea’s) are ‘hybrids’, meaning that they have a mix of foam and pocket springs. Having some sort of ’springs’ in the mattress does make it easier to turn. Don’t fall for promises of great memory foam that is cheap. In my opinion, cheap memory foam breaks down pretty quickly, leaving you with problems.
So… if you feel that you may need a change of bed or mattress, go to a good bed shop and lie on loads of different beds. Be prepared to spend a bit of time to get a feel for different beds. If you are buying just a new mattress, make sure you try the mattress on the same type of bed base that you already have at home.
If you have pain at night that is not going away or in-fact, getting worse maybe sure you see a health professional to determine WHY are in pain at night. Don’t just leave it.
This is also a useful link on How to Choose a Mattress from The Sleep Foundation.
We have an amazing team of Osteopaths and we also have a great massage therapist and reflexologist.
Call us on 020 8605 2323 if we can help.
Blog post by James Dodd

Bone Stress Injury
A bone stress injury (BSI) is due to a bone’s inability to cope with repetitive mechanical loading.
This results in structural fatigue with localised bone pain and tenderness.
Essentially, BSI is an overuse injury and is normally multifactorial with a combination of biological, biomechanics and anatomical risk factors.

A bone stress injury (BSI) is due to a bone’s inability to cope with repetitive mechanical loading.
This results in structural fatigue with localised bone pain and tenderness.
Essentially, BSI is an overuse injury and is normally multifactorial with a combination of biological, biomechanics and anatomical risk factors.
Lower limb stress factors are much more common than upper limb stress factors. Tibial stress fractures account for approximately half of all stress fractures, followed by the forefoot and then femoral shaft and neck.
It can be broken down into extrinsic and intrinsic factors:
Extrinsic factors:
Training errors
Excessive volume
Excessive intensity
Sudden change in intensity
Poor recovery
Excessive fatigue
Surface
Hard/soft/cambered
Shoes
Poor shoes/worn shoes
Equipment
Inappropriate kit
Poor nutrition
Psychological factors
Environmental conditions
Intrinsic factors:
Training errors
Pes planus/cavus
Hip anteversion
Leg length
Muscle weakness/imbalance
Lack of flexibility
Genetic factors
Endocrine factors
Metabolic factors
RED’s
Previous bone stress
Smoking
Family history
The management of BSI begins with off-loading the affected bone to reduce pain and assist healing. A holistic overview is taken to improve general wellness including sleep and nutrition. This is complemented with a gradual loading programme with physical therapy.
Rapid and clear diagnosis is essential in preventing the propagation of the fracture.
To assess the history of the BSI we will need to know:
The type of impact sport/physical activity you’ve been doing
Any changes in intensity, frequency, time, environment
Changes in the recovery
Any female REDs (relative energy deficiency)
Your general nutrition
Where the pain is, especially when loading, e.g. for a lower limb we’d look at where the pain is when running or hopping
The point you feel the pain will help decipher how long you have been suffering with that stress fracture. Early stress fractures often give pain towards the end of an activity, whereas with more well established BSI, pain comes on earlier on, or even at rest. It can also be more intense and linger for longer in more established BSI.
Examination
To examine a BSI we would look at a number of things, focal tenderness and swelling on palpation, percussion may reproduce the pain. We would look to run a tuning fork test and a fulcrum test. For lower limbs we’d look to see if you can stand on one leg and see if you can hop on the affected leg.
Imaging
Often an x-ray will suffice to view a stress fracture, although it can take 2-4 weeks for it to show on x-ray and sometimes cannot be seen at all. If it cannot be seen we can use a bone scan - the downsides of this is they are time-consuming and involve an injection and exposure to radiation. An MRI is sensitive and specific for BSI, it gives a very accurate correlation to the picture. It can be costly though.
Management for BSI
Offload/stop participating in activity, especially high impact exercise
Maintain fitness levels through cross training - swimming, cycling, pool running
Consider immobilising your injury - e.g. using a brace
See an Osteopath who can work with you to gradually strengthen and improve flexibility
Address any dietary needs
Ca and Vitamin D supplements will help improve any bone issues and deficiencies
Look at hormonal balance for those who may suffer from a hormonal dysfunction
Address REDs if necessary
If you are concerned about an injury, BSI or other, please give us a call today on 020 8605 2323.
Blog post by James Dodd

Chronic Heel Pain; Is it Baxter’s Nerve Entrapment?
Sufferers of chronic heel pain often are often diagnosed with Plantar fasciitis, however not all cases of heel pain are due to this. Other causes include nerve trapping, joint inflammation, stress fracture and Baxter’s nerve entrapment. In fact, Baxter’s nerve entrapment can cause up to 20% of cases of chronic heel pain.



Do you suffer from Chronic Heel Pain?
Sufferers of chronic heel pain often are often diagnosed with Plantar fasciitis, however not all cases of heel pain are due to this. Other causes include nerve trapping, joint inflammation, stress fracture and Baxter’s nerve entrapment. In fact, Baxter’s nerve entrapment can cause up to 20% of cases of chronic heel pain.
So, what is Baxter’s nerve?
Baxter’s nerve is a tiny nerve coming from the larger plantar nerve on the inside of the ankle. It supplies the small muscles of the foot and sensation to the heel. When the nerve becomes impinged it causes a sharp, burning pain, often associated with pins and needles and numbness and pins around the heel.
What causes Baxter’s nerve entrapment?
Baxter’s nerve entrapment can occur after injuring your ankle or heel, but more commonly, it develops slowly, without injury. It is unclear how it happens but there are theories that the nerve might become trapped from pressure, due to reduced movement of the ankle joint, flattened feet, and/or a pressure from a heel spur or plantar fasciitis. It can happen to anyone and doesn’t appear to be gender or age specific.
What are the symptoms and diagnosis
Symptoms often include:
Pain when you touch the inside of the heel
A sharp/burning pain around the inside aspect of the heel
Pain when walking and placing your foot on the floor after a period of rest
Some people may suffer from pins and needles around the inner aspect of under the heel. Especially when the nerve is knocked or trapped.
Although Baxter’s nerve entrapment presents very similarly to plantar fasciitis, there is a subtle difference in where the pain is felt and some of the symptoms. Baxter’s nerve entrapment is felt on the heel and the medial arch of the foot, whereas Plantar fasciitis is more concentrated just on the heel. As noted above Baxter’s nerve entrapment can also include a sensation of numbness or pins and needles.
Imaging such as ultrasound or MRI can help with diagnosis. You might see thickening of the small Baxter’s nerve on the inside of the heel, or if your scan appears normal this increases suspicion of nerve trapping as the cause of pain. In severe cases, nerve trapping can cause shrinking of the muscles on the outside of the foot which will be seen on MRI.
What is the treatment of Baxter’s nerve entrapment?
Often, we would start with simple, gentle treatments, such as taping and orthotics (inner soles for your shoes), stretching and foot strengthening. We would give an individual strengthening routine and specific stretches to work on at home. Sometimes an injection of cortisone can be helpful, this would be done with ultrasound to ensure we target the correct site of Baxter’s nerve trapping. Finally, in some cases, surgery to release the Baxter’s entrapment might be needed.
If you are suffering from any form of heel pain, get in touch with the team today and see what we can do to help you.
Blog post by James Dodd

CANCANEAL APOPHYSITIS (SEVER’S DISEASE)
This is painful inflammation of a child’s growth plate at the heel. Normally, this affects children between 8 – 14 years old as their calcaneus (heel bone) is still developing.

This is painful inflammation of a child’s growth plate at the heel. Normally, this affects children between 8 – 14 years old as their calcaneus (heel bone) is still developing. It is also at a time when children often increase the amount of exercise they do. With increased and repetitive use, the achilles tendon ‘tractions’ on the growth plate at the heel and so causing pain and inflammation. Approximately 60% of Sever’s is bilateral.
Causes
It is essentially an overuse injury at the time of growth. Sports that ‘load’ the achilles tendon and heel such as running and jumping are normally the culprits. Often a bout of Sever’s can become aggravated at the start of a season after a ‘rest’ period or exercising on harder ground as it gets colder. Tightness in the calf can also lead to increased load onto the heel bone. It bad cases, it may take until the child stops growing before complete resolution. It is also really important to try to observe why there has been more load placed onto their heel… this may be from a stiff hip or other area. This is key to successful treatment.
Diagnosis
This needs to be based on a full and correct examination by your osteopath, doctor or other medical professional. X-ray or MRI may be used to confirm the diagnosis or monitor the progress, but often this is not necessary.
Treatment
Calcaneal apophysitis has no known long-term complications and is self-limiting; that is, it should go away when the two parts of bony growth eventually join together (occurring around 16 years of age).
It is important to limit (temporarily) excessive or rigorous activity in its painful stages. But it is also about management, as you can get times when it calms and at other times, it can then flare up again as they increase activity. Soft shoes and heel cups can make a difference and it is important to make sure the child has sound biomechanics (eg no excessive pronation or muscular imbalance). Regular and correct stretching of the tight muscles in the calf and thigh are essential. Ice can be of great help if used correctly. Anti inflammatory medication may be of use – but do check with your medical professional about this first.
Seeking help from your osteopath or good physical therapist can really help too. They will check for poor biomechanics and work and stretch the calf and thigh and manage this injury with some good strengthening exercises.
Return to sports or activity
The goal here is to get your child back to their desired sport or activity as soon as safely possible. It may be a gradual return to see if the condition regresses. If they return too early, it may lead to more chronic pain.
To return to sport your child should have no pain at rest and should be able to walk pain free. They should also be able to jog, sprint and hop pretty much symptom free too.
If after the pain resolves…. it is important that there is still a regime of regular stretching of their calves, thigh and leg muscles.
Blog post by James Dodd
Strength is often forgotten and sarcopenia
Strength is SO often forgotten in place of the need to stretch!
This post is about strength. Strength is important. Strength is SO often forgotten in place of the need to stretch!
How many times have you been in the garden for a few hours or been doing DIY and the next day you are struggling to move? Often I ask people how they have prepared themselves for this amount of bending or DIY under load and they look at me as if I am mad! They then tell me that they sit at a desk all day and all week.
To enable our bodies to cope with bending for an extended period of time, lift things that we are not used to or even to bend and reach in a new way…. we NEED to have the capacity in our body to cope this. Claire Minshull had a lovely way of describing ‘capacity’ and she compared it to a fuel tank. She said that if your fuel tank is full, you should have good power, but if it is almost empty, you may well struggle to do pretty basic things.
Capacity is strength!
Capacity gives you more endurance.
Capacity helps you to do more.
Stretching will help you to move better to new places, BUT it will not give you more capacity to lift and bend in a sustained way. It not give you more endurance. STRENGTH or increased capacity will.
As we beautifully age…. and become less active, many of us get Sarcopenia.
The definition of Sarcopenia is the loss of skeletal muscle mass and strength as a result of ageing. The main reason for this outside illness is living a sedentary lifestyle which many of us have. We do more sitting and generally do less. Getting little or no physical activity on a regular basis puts people at an increased risk of developing sarcopenia as they age.
Can we do something about us having or getting sarcopenia? Yes!!
There is an important correlation between inactivity and loss of muscle mass and strength. This suggests that physical activity should be a protective factor for the prevention but also the management of sarcopenia. It gives you greater control and will be protective against things like falling.
As you get stronger, the stairs become easier, getting up from a chair is so much easier, as is getting off the loo or up off the floor.
So, if you are tending to be very sedentary or struggling to get the motivation to do more to help your self, get some advice of how to get moving more and maybe even to start to add load to your system to keep your muscles and bones strong. It is great for the health of our bodies and helps with longevity.
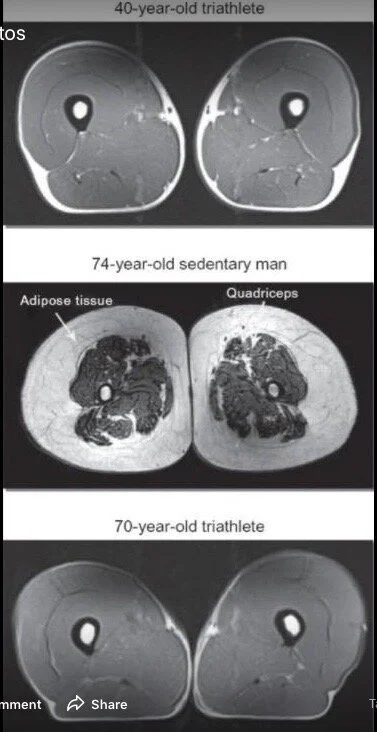
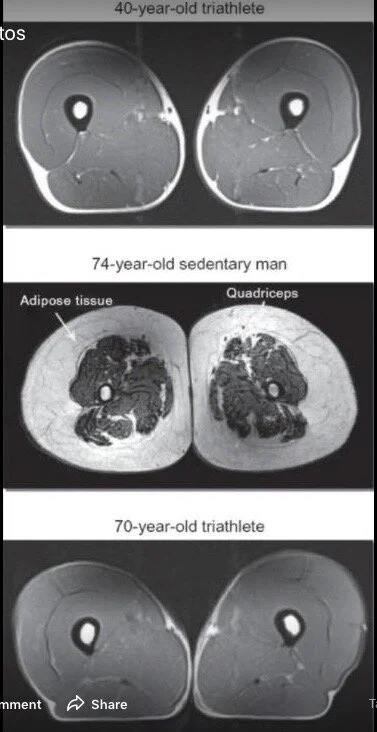
See below. The picture at the top is a fit 40 year old. The picture at the bottom is a fit and strong 70 year old. Then picture in the middle is a normal 74 year old. One that does very little. Probably watches a lot of TV and reads a lot. You can see the massive muscle wasting and this has been replaced by fat. The middle man is not fat. He just has much less muscle mass. So he will struggle to do much. Stairs will be hard and so will getting up from a chair.
You don’t have to go to the gym for hours to achieve this. But you do need to challenge your bodies a bit. Starting gradually and build. Start with longer walks and then walks up and down hills. If you are unsure about this, get advice from a medical professional.
It is all about choices. But this is one choice that most of us can make with a positive end result.
If you want some help with this, call the team at Back to Back on 020 8605 2323.
Keep fit and well and STRONG.
Blog post by James Dodd

RED-S or RELATIVE ENERGY DEFICIENCY IN SPORT
You need to have sufficient calories or energy to meet the demand of high level activities or sports. If you do not get enough, any number of problems can start.

Just a great Podcast to listen from Physio Matters.
Really highlighting that you need to have sufficient calories or energy to meet the demand of high level activities or sports. If you do not get enough, any number of problems can start. A must listen session regarding an important issue with take home messages much more wide reaching than just for this condition and some real clinical pearls from the outset. Therapists, coaches and managers must be more aware of this!

Low carb vs low fat for Type II diabetes
Diabetes can be utterly destructive and many just think taking pills that a doctor gives you will sort the problem. It does not!! It only treats the symptoms and does nothing to sort out the disease.

Have a listen to this two-part podcast that talks about the research into low carbohydrate and low fat diets in the management of type II diabetes. In part 2 of the podcast, it discusses more on nutritional advice for the management of type II diabetes.
How a read and empower yourself with the knowledge it gives you to either help yourself to offer advice to someone in need.
Diabetes can be utterly destructive and many just think taking pills that a doctor gives you will sort the problem. It does not!! It only treats the symptoms and does nothing to sort out the disease.
Some of the management of this massively difficult problem is about the need to change and adapt dietary choices, but it is also important to make good lifestyle choices such as taking regular exercise, improving the amount and quality of sleep you get and managing one’s level of stress.
LINKS
If you need any help with the above subject, see your doctor or a good healthcare provider with an interest in the subject.
Blog post by James Dodd

Sleep – are you getting enough or enough ‘good’ sleep?
SLEEP is much more important than most of us think. It is actually a massively crucial time for our bodies to rest and heal and for us to lay down new tissue. It is also an important time for our brains to process what has happened that day and ‘back up’ its new memories.

SLEEP is much more important than most of us think. It is actually a massively crucial time for our bodies to rest and heal and for us to lay down new tissue. It is also an important time for our brains to process what has happened that day and ‘back up’ its new memories.
An adult should be getting 7-9 hours sleep a NIGHT!!
Here are ten tips to try and improve your sleep. I hate the phrase Sleep hygiene.
Try to do all of some of these. The more regularly you do them the better. Some will be hard to do all the time, but try to do at least 3-4 times a week. Sleep helps us function better and improved sleep helps with stress levels.
Sleep in a dark, quiet and cool room.
GO ‘device free’ at least one hour before bed
Use bedroom for sleep only (other than the obvious!!)
Nap wisely (before about 3pm) but do not look at naps badly.
Get out of bed if you cannot sleep (use the 20 minute rule)
Maintain a consistent, regular bedtime routine
Do not go to bed hungry
Finish exercise at least 3 hours before bedtime
No alcohol or nicotine for 3-6 hours before bedtime
Stop caffeine 6 hours before bedtime
Back pain and a large number of other conditions have been closely linked to poor sleep.
For more information look to
The Sleep Society and the The Sleep Council
https://www.sleepsociety.org.uk
Blog post by James Dodd

Syndesmosis injuries are often missed and why…
Syndesmosis injuries do happen and they probably happen more than we think. They are often missed and are treated as a ‘normal’ lateral ankle sprain.

Syndesmosis injuries do happen and they probably happen more than we think. They are often missed and are treated as a ‘normal’ lateral ankle sprain.
Anatomy
You have two bones in your lower leg, the tibia and the fibula. The point just above the ankle where these two bones meet is called the syndesmosis. The tibiofibular syndesmosis is a fibrous joint joining the fibula to the tibia and stabilized by four lateral ligaments: the anterior inferior tibiofibular ligament (AITFL), the interosseous ligament (IOL), the transverse ligament (TL), and the posterior inferior tibiofibular ligament (PITFL)
An ankle syndesmosis injury is often called a ‘high’ ankle injury or sprain. It can be missed in the early stages as the amount of pain and swelling is not always proportionate or may not reflect the severity of the injury. Swelling can often be much less that the ‘normal’ ankle sprain. Remember ‘a simple ankle sprain’ is not always ‘a simple ankle sprain’.
Patients with a syndesmosis injury will describe a mechanism different to a lateral ankle sprain in that they did not roll over on their ankle. Pain is often felt above the lateral malleolus, but they may also feel medial ankle pain in a severe injury.
One of the most common mechanisms of this injury is with forced external rotation and dorsiflexion at the ankle. This is often with the foot caught on the floor and the knee is forced forwards and around.
Ankle Sydesmosis injury Classification
Grade I AITFL – an isolated injury
Grade II AITFL and interosseous injury
Grade III AITFL, PITFL and interosseous injury
Grade IIII AITFL, PITFL and interosseous injury as well as the deltoid ligament.
With grade I injuries, there is a degree of pain, but they are not unstable and can be managed in a way similar to that of a grade I MCL injury with strapping and a short period off sport.
Grade II requires experience to differentiate between a stable and unstable. Grade III and above is normally managed with surgical intervention.
Tests
Reliable tests for syndesmosis injuries are a few, but the most sensitive is the hop test.
Others are ‘knee to wall’ test, ‘Dorsiflexion/external rotation’ test, palpation of the ligaments, ‘squeeze test’, ‘fibular translation’ test and ‘anterior draw’ test. Remember that no test in isolation is good enough for diagnosis.
Acute Management
I am not going into the treatment of this sort of injury, but great advice that seems to be consistent with some experts is to put people into a boot when you suspect a syndesmosis injury. This immobilises the ankle and you can modify weight bearing for the first 24-48 hours. This just gives this area a chance to calm before treatment commences. This improves the reliability of the examination by waiting for the initial pain and inflammation to settle. A management plan can then be made.
Treatment must also involve the rest of the body, not just the poorly ankle. Integration of the knee and hip along with the rest of the body encourages better and faster return to sport.
Further Reading
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4128849/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4094093/
https://www.ncbi.nlm.nih.gov/pubmed/26725452
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5370648/
If you are struggling with an ankle injury – get it properly assessed and treated. If you would like to see one of our sports osteopaths, call 020 8605 2323.

Achilles Tendon Pain
Achilles tendon pain - examination, tests and rehabilitation thoughts.

Here are some really interesting snippets about Achilles Pain.
EXAMINATION
The assessment must include a thorough case history and examination and one is needing to establish the site of pain and the aggravating and relieving factors.
One of the main aggravating factors that fit a ‘tendon pattern’ is pain with increased load. This may be during or after exercise. The site of pain is localised around the achilles tendon, normally 2-6cms from the insertion. The patient will often point to where they feel their pain. There may or many not be swelling or a ‘bump’ on or around the tendon.
TESTS
Other than observation and palpation, there are a couple of really great tests. The London Hospital Test and the Painful Arch Sign.
The London Hospital test is where the clinician pushes on the sore area and then passively dorsiflexes the ankle and then pushes on the tendon again in the same place. A positive test is where there is a reduction in pain. Tendon expert Seth O’Neil feels that this finding is due to the additional stretch to the tendon tightens the exterior of the tendon and this protects the interior or deeper parts of the tendon. The deeper areas are where most achilles problems stem from.
The Painful Arch Sign is to distinguish between a tendon and a sheath problem. By gripping the swollen area and then dorsiflexing the ankle the clinician is looking to see if the swelling is moving as you move the ankle. If it does move as you move the ankle, it suggests a tendon problem. If it is a sheath problem, the swelling should not move.
You do need to exclude all other pathology. One of the most common differential diagnosis of Achilles Tendinopathy is posterior ankle impingement. This clip shows you how to examine for this. But there are still many other causes of pain to the back of the heel and these do need to be ruled out.
People normally get some sort of achilles pain when they have increased the demand on these tendons over and above what their bodies are able to adapt to.
REHABILITATION THOUGHTS
Advice on how to rehabilitate these no longer invoices trying to stretch the tendon. They now know that in Achilles Tendinopathy, the tendon becomes more pliable and so does not need to become more pliable. We need to try and help it to become stiffer again. The soleus is often more involved with achilles tendinopathy than the Gastrocnemius.
The main model of rehabilitation is about load using eccentric and concentric and isometric. These may be used at different stages of the treatment depending on how reactive the tendon is. It is often found that there is a great deficit in power in those with achilles tendon problems.
Studies have shown that tendon stiffness does increase with resistance training. One study mentions a 19% increase in stiffness after 8 weeks. But the load needs to be progressive towards 80% of the patient’s one rep-max (1RM). This will need to happen over time. With lower loads of 20% of 1RM, they saw no adaptation in the tendon. When returning patients to high level activity, rehabilitation should incorporate external loads of at least 50% body weight. That is key and super interesting!!
The soleus is predominantly involved in Achilles tendinopathy and should she it should a large part of the target of rehabilitation.
It may be appropriate to perform exercises 3 times per day for both sedentary and the athletic population. This is based on data looking at the response of bone cells to loading in osteoporosis. Bone cells peak at around 45 hops and are stimulated for 5-6 hours after loading. This is probably similar for tendon cells as they are derived from the same cells (fibroblasts). SO don’t overdo the load – but trying towards 3 times a day certainly makes scientific sense.
BE gradual when increasing the load. Don’t add too much much weight too soon or it will make you sore and do work within your patterns of soreness.
Being patient with longer standing achilles problems is REALLY key.
Depending on the severity of the tendonopathy, it could take a few months to get really good adaptation back in the tendon, although you should feel good changes in 3-6 weeks.
Here at Back to Back, we really feel it is critical that you DO NOT look at the Achilles Tendon in isolation! Foot function, whole leg function and how well the same side hip and the opposite hip load and unloads often highlights as to why there may have been a problem to start. Observation of these must be part of you assessment and management , NOT just your sore achilles tendon.
If you need some help with rehab or what to talk to one of our great sports Osteopaths, call the clinic on 020 8605 2323. Before embarking on any heavy loading, do ask a health professional.

Sever’s Disease. Heel pain in children.
Essentially, it is an overuse injury at the time of growth.
Sports that ‘load’ the Achilles tendon and heel, such as running and jumping, are normally the culprits. Often a bout of Sever’s can become aggravated at the start of a season after a ‘rest’ period, or exercising on harder ground as it gets colder.

Causes
Essentially, it is an overuse injury at the time of growth.
Sports that ‘load’ the Achilles tendon and heel, such as running and jumping, are normally the culprits. Often a bout of Sever’s can become aggravated at the start of a season after a ‘rest’ period, or exercising on harder ground as it gets colder. Tightness in the calf can also lead to an increased load on the heel bone. In bad cases, it may take until the child stops growing before complete resolution.
Other important areas to look at as to ‘why’ this may have happened, are ankles that do not move well and/or feet that are stiff which result in the force from the ground being poorly dissipated.
Also hips that are unable to give the range of movement required can increase the load to the achilles and heel bone, leaving the heels to take the hit! This is key to successful treatment. The symptoms and the diagnosis is Severs Disease, but it is not telling you ‘why’ this is happening.
Diagnosis
The diagnosis of Sever’s Disease needs to be based on a full and correct examination by your osteopath, doctor or other medical professional. An X-ray or MRI scan may be used to confirm the diagnosis or monitor the progress, but often this is not necessary.
Treatment
Calcaneal apophysitis has no known long-term complications. This is self-limiting in that it should go away when the two parts of bony growth eventually join together (occurring around 16 years of age).
It is important to limit (temporarily) excessive or rigorous activity in its painful stages. This needs to be about management, as you can get times when it calms and at other times when it can flare up again as they increase activity. Soft shoes and heel cups can make a difference. It is important to make sure the child has sound biomechanics (e.g. no excessive pronation or muscular imbalance). Regular and correct stretching of the tight muscles in the calf and thigh are essential. Ice can be of great help if used correctly. Anti-inflammatory medication may be of use, but do check with your medical professional about this first.
Seeking treatment from your osteopath or good physical therapist can really help too. They will check for poor biomechanics, work and stretch the calf and thigh, and manage this injury with some good strengthening exercises.
Return to sports or activity
The goal here is to get your child back to their desired sport or activity as soon as safely possible. It may be a gradual return to see if the condition regresses. If they return too early, it may lead to more chronic pain.
To return to sport your child should have no pain at rest and should be able to walk pain free. They should also be able to jog, sprint and hop pretty much symptom free as well..
After the pain resolves it is important that there is still a regime of regular stretching of their calves, thigh and leg muscles in place.
If you have any questions or would like us to look at your musculoskeletal problem, please book in to see an osteopath at Back To Back on 020 8605 2323.
If you suffer from an acute muscle injury and are not sure what to do, it is always suggested that you see your GP, Osteopath or Physiotherapist for further assessment and advice on treatment and management.

Do you get pain when playing golf?
At Back to Back we treat more than a few golfers and their injuries. An injury common to the golfer may be one of many…. But often a golfer presents with pain in their elbow, shoulder, their back, hip or knee. Pain is all too common in golfers!

At Back to Back we treat more than a few golfers and their injuries. An injury common to the golfer may be one of many…. But often a golfer presents with pain in their elbow, shoulder, their back, hip or knee. Pain is all too common in golfers!
Identifying with their pain can be the easy part. Working out why they have pain is often a little more challenging.
Assessment of injuries
Our AFS (or Applied Functional Science) team will be best to do this. Their aim is to track down the ‘why behind the what’. What I mean by this is … why has that particular area of your body failed? Which area in that person’s body is not working as it should and increasing the ‘load’ elsewhere?
I saw a patient last year and remembered this all too common story. He was in his late forties with a handicap of 4! He had been suffering with right shoulder pain for the previous 5 months! He had seen a few other practitioners before finding his way to the clinic.
To me, it was crucial to see him swing as if he was hitting the ball! Watching this and adapting the way he hit the ball, it immediately became apparent that he was restricted in his left hip. As he was halfway through his backswing the movement that should have been available at his left hip was not there and he was then using his upper back and right shoulder to do much more work than it needed or was build to do.
All that was happening was his shoulder was becoming strained because of his hip! Before coming to see us, this lovely patient had had his shoulder and surrounding area rubbed for 14 treatments. Working with his left hip and left foot and integrating them into his swing gave great results in 3 treatments and he was almost pain free at 4 treatments. He still has a small way to go, but it just goes to show that rubbing symptoms (in this case the shoulder) is not always the right answer. Getting fully assessed by someone that appreciates integrated movement and treats the body as a whole is critical.Get assessed properly and get properly fixed!

Could your groin injury be coming from your hip?
Groin pain can be a difficult problem for patients as well as their clinicians. Part of the problem is that the location of the pain is often a poor indicator of the where the pathology actually lies. Additionally, when the pain becomes chronic, multiple pathologies can be generated, adding a further layer of complexity.

Groin pain can be a difficult problem for patients as well as their clinicians. Part of the problem is that the location of the pain is often a poor indicator of the where the pathology actually lies. Additionally, when the pain becomes chronic, multiple pathologies can be generated, adding a further layer of complexity.
It is very important to make a clear diagnosis. We should seek to look beyond merely labelling the problem as a ‘groin sprain’. There many causes of pain in the groin. Approximately 50% of groin pain can be attributed to pain generated by the hip joint; a surprise, perhaps, for younger patients. As in any medical condition, the patient’s history will give us many clues. It is extremely important to rule out sinister ‘red flags’. These could be night pain, severe pain on loading the leg, weight loss or systemic symptoms, and we need to be mindful of conditions which may occur in certain age groups, such as a slipped epiphysis in teenagers.
Common causes of groin pain besides the hip, include those generated by the lumbar spine, pubic overload (osteitis pubis), iliopsoas and adductor tendon pathologies. You need to be aware of stress responses in the femoral neck in runners. Abdominal wall hernias may cause pain which is a little higher in the groin. Less commonly, younger patients can experience the rectus femoris pulling away from its attachment at the anterior inferior iliac spine. Testicular tumours and avascular necrosis can present insidiously and we need to be on the lookout for them.
A big proportion of patients who present with groin pain as a result of hip pathology, have an underling condition known as ‘femoral acetabular impingement syndrome’, or FAI. This is essentially a problem resulting from a tear in the acetabular labrum, usually caused by repetitive trauma. This may be due to a ‘bump’ or ‘CAM’ on the head neck junction of the femur, which may be acquired or genetic.
This can cause groin pain which is worse with exercise, sitting or standing. The pain can be brought on by putting the patient in the ‘impingement position’ of hip flexion + internal rotation + adduction. In the long term, we believe that the tear in labrum causes changes in the acetabular articular cartilage next to it, and over many years, this may lead to osteoarthritis in the hip.
FAI can affect people of all ages, and is often missed in 30-40 year olds. Taking a careful history, and carrying out a thorough examination can help identify the likely cause. Imaging, such as 3t MRI of the hip, can help confirm the underlying diagnosis (as X-Ray cannot rule out FAI). It should be remembered that imaging needs to be interpreted in light of the history and examination findings. FAI may require treatment with hip arthroscopy surgery, but in some cases injection therapy and robust physiotherapy or osteopathy may be enough to get a person back to full activity.
Sports Physicians and Osteopaths are ideally placed to identify the underlying cause of unexplained groin pain, and are skilled in directing the rehabilitation necessary to resolve the problems.
If you have any problems at all and would like in to see James Dodd or one of the team at Back to Back, please call 020 8605 2323.

1080 Map Functional Assessment
Developed in Norway and Sweden, 1080 Map Functional Assessment is a specialist assessment tool with software that is designed specifically for those committed to becoming more successful in their training and to improve their movement patterns.
James at Back to Back is now offering an exciting new service called 1080MAP™. Developed in Norway and Sweden, it is a specialist assessment tool with software that is designed specifically for those committed to becoming more successful in their training and to improve their movement patterns. It is also a great tool to be used alongside rehabilitation protocols.
1080MAP™ assesses, analyses and optimises movement patterns to maximise your physical performance. There really is nothing like this in the world that assesses and maps out your movement patterns and using specialist software, it gives clear results to show how well your body moves! At the time of writing, there are only a couple of people with specialist training in London to do this and we have been lucky enough to be part of this.
This functional assessment is a unique, effective and accurate test system for determining a person’s fundamental ability to move and control movement. The system is based on combinations of full-body movement patterns that give results that will determine what may be needed to improve athletic ability or everyday function.
The first level of 1080 MAP covers mobility and stability as this is the foundation of any human movement and physical performance.
To measure full-body three dimensional movement patterns the 1080 MAT is an easy-to-use tool. It consists of a circular test area divided by vectors. Measurements in centimetres and degrees provide the input to the 1080 MAP database.
1080 MAP stands out as the only scientifically validated method that is repeatable for mobility and stability assessment.
Assessment
The measurement of movement patterns in standing positions to quantify function. Quantification of mobility, stability, strength, power, endurance and performance.
Analytics
The different tests are scored are then combined and directly linked to each other to create unique individual profiles. All profiles reflect physical performance, identify physical limitations and hidden potential.
Optimisation
1080MAP™ results in highly specific and individualised treatment and training programs that will optimise functional performance.
The picture below is the 1080Map of an elite athlete who was struggling with lower back pain for years. The graphic below shows some of the information we produced. It highlighted problems with her left hip (from left picture) and foot that had not been seen from previous assessments. The new and crucial information was then used in her treatment plan to target her left hip and foot. These were integrated into her movement patterns. She now is able to run really good distances and she is stronger with much less pain.
Test results are captured, analysis is done, and feedback is given from the 1080 MAP cloud based client management system. Here, each client’s results can be compared over time, on detailed level or by using a composite mobility score. Comparisons can also be done against the entire data base population based on gender, age, sport and performance level. Based on the analysis, feedback can be sent directly to the client.
If this could be something of interest to you, call the clinic on 020 8605 2323 and book into see James for a 1080 map assessment. Here is a link to more information. Our website also gives you information about the clinic.

Loosing the boozing-reduce your Alcohol for a healthier you
Although you may first visit your osteopath to treat an injury or condition, a priority of the osteopath is to help you improve your overall health and wellbeing.

Alcohol after a busy Festive period
Although you may first visit your osteopath to treat an injury or condition, a priority of the osteopath is to help you improve your overall health and wellbeing.
There are a range of things that we do to our bodies that can help or hinder this, such as exercise and diet. Another significant factor is alcohol consumption.
With the new year underway, you may be looking to kickstart 2018 with a range of healthier living decisions. You may be trying the ‘Dry January Challenge’, to go without alcohol for a month. Or maybe you are looking to reduce how often or how much you drink.
If you experience joint pain, excessive alcohol can impede your bodies ability to repair and also interact badly with some medication.
Long term excessive drinking can also cause:
*Brain damage
*Increased risk of throat and mouth cancer
*Increased blood pressure and heart disease
*Inflammation of the stomach lining, stomach ulcers and increased risk of stomach and bowel cancer
*Liver damage and cancer
*Reproductive problems
*Mental health difficulties
Blog Post by James Dodd

The endangered glutes!
There’s a fairly obvious giveaway about the importance of our gluteal muscles; they are rather big! Having a big, powerful set of muscles such as the glutes should indicate to us that, through our evolution, the body has developed a demand for strength and power in that area.

Why are they not firing and what to do about it.
There’s a fairly obvious giveaway about the importance of our gluteal muscles; they are rather big! Having a big, powerful set of muscles such as the glutes should indicate to us that, through our evolution, the body has developed a demand for strength and power in that area.
Human anatomy has evolved to cope as efficiently as possible with the forces exerted upon it. Perhaps the most important force of all is gravity. Every time you take a stride, or step off from a curb, or land from a jump, there is a demand for the body to control this movement. Without our muscular system engaging to catch us, we would collapse like a bag of bones under the force of gravity.
The most powerful hinge in the body, which has evolved to adsorb these forces, is the hip. It makes sense, therefore, that the hip would need a big set of muscles surrounding it in order to absorb these forces and exert the control that is required – hence the big glutes!
Having developed a powerful set of muscles such as the glutes, it would be efficient for the body to regularly recruit their power when performing tasks. If I want to perform a movement efficiently, such as bending down to empty the dishwasher, I would like the powerful parts of my body to control this movement – rather than the smaller and more vulnerable muscles.
If we don’t use the large muscle groups appropriately, then smaller muscles may be asked to do more work and may end up failing.
The importance of the glutes is widely recognised and often discussed in gyms and clinics all over the world. You may have even been told that “your glutes aren’t firing” and may be currently trying to rectify this! Unfortunately, however, the glutes are often blamed (and trained) in isolation.
A lack of understanding of how the glutes work, leads to a very limited approach to gluteal training. The important question to ask is; why are the glutes not firing? Only by answering this will you be able to improve your gluteal activation and strength.
So, why do so many of us under use our glutes and how do you actually get them to work harder for you?
Evolution lesson #1 – use it or lose it!
I always feel that any announcement to a patient that “your glutes aren’t firing” should be delivered with a caveat. The caveat being that, for most of us, this is simply a bi-product of our modern lifestyles, it is not an unfortunate affliction that you just happen to be unlucky enough to have developed. Don’t worry; we’re all in the same boat. It’s not your fault!
A quick look at the animal kingdom can help to explain this point. Often we identify animals by their anatomical features, without necessarily knowing that we do so. If I asked you to look at the images below of the Capuchin Monkey and the Springbok and tell me where their “big bits” are, then I’m hoping you would say the Capuchin’s tail and the Springbok’s hind legs.
Even without knowing the habits of these animals, you would probably be able to make a fairly good guess as to what they were good at. The monkey has a powerful tail for climbing and swinging from trees, the Springbok has big hind legs for jumping.
Their anatomy has evolved to be fine-tuned for their lifestyles, habitats and activities and their continued success as a species is dependent upon them using these powerful areas to gain advantages in the wild. These animals take maximum advantage of their powerful areas!
This is where the problems for humans arise. We are far more sedentary now than at any time during our evolution. For many of us, the continued demands required to maintain the strength and power of our big muscle groups has significantly reduced. Our anatomy has been fine tuned to cope with regular, unpredictable, multi-directional movement such as jumping, landing, walking on uneven ground, running, sprinting, changing direction. By sitting, moving less and existing in very flat, unchallenging habitats we are no longer putting these demands on our bodies.
The gluteal muscles fire when they are placed under load through movement combined with the forces of body weight and gravity. They respond to three dimensional movement, so not just up and down, but side to side and rotational movements. We, not only, have a habit of being too sedentary but also training and exercising in a very one dimensional fashion. This leaves our glutes fairly underwhelmed.
So, how do we actually get the glutes to fire?
Although there is no literal need to throw out the trappings of modern life and return to an animalistic state in order to rescue our glutes, there may be a figurative one.
The best way to get the muscular system to activate, and to make any long term changes to the firing of muscles, is to make them do authentic movements. It is crucial for us to really understand what the gluteal muscles have evolved to do.
The glutes are designed to slow down and control our hip movements, both from the ground up and the top down.
Every time our foot hits the ground, the forces from above and below place a huge demand on our hips and the large glutes are there to cope with this significant work load. As the hips absorb movements such as landing or squatting (combined with gravity), the glutes fire in order to control this movement and convert these forces into elastic and kinetic energy. This energy is then utilised to fire us off into the next part of the movement, whether it be the next step or a jump from our squat.
If we want to train the glutes, then we need to create authentic movements at the hip. Only then will the nervous system recognise the movement and create the appropriate activation.
Glute bridges don’t cut it.
If you have been told that you have lazy glutes then you may currently be doing regular glute bridges to switch the blasted things back on again. This is where you lay on your back with your knees bent and lift your pelvis towards the ceiling.
Although this will indeed shorten the glute muscles and may cause them to fatigue – it is by no means an authentic movement. A glute bridge is not something that you are really required to do in daily life.
Putting one foot out in front of you, while reaching forward to pick something up is an action you are required to do frequently. Landing on one foot, while rotating your upper body, is a movement that you do every time you walk. By exercising and challenging the hips in these authentic positions, we begin to re-educate the glutes as to their true purpose. Our nervous systems are very plastic; they have the potential to adapt quickly. If we actually encourage the body to move in the way that it is designed to, our nervous systems will soon catch on to what we are asking of the body and begin to adapt and create the appropriate firing of muscles. If we continue to train in a non-authentic way, our nervous systems will remain confused and will seek ways of compensating – often leading to dysfunction.
Blog post by James Dodd

Standing desks…… a small note
I have just seen an article written in The Times yesterday by Carol Midgley on the subject of standing desks.
She talks briefly and mentions that ‘sitting is the new smoking’ and so she tries a basic device. This new device, you sit onto your existing desk to enable you to stand and work. I am not sure which one she tried, but here is a great example.

I have just seen an article written in The Times yesterday by Carol Midgley on the subject of standing desks.
She talks briefly and mentions that ‘sitting is the new smoking’ and so she tries a basic device. This new device, you sit onto your existing desk to enable you to stand and work. I am not sure which one she tried, but here is a great example.
She says “So after a few days of spending eight hours of standing, am I convert?” “No.” “Not one iota.” She talks of it being harder to focus and harder on ‘the old plates of meat’.
When you start to run, you do NOT just go out and run for 2 hours! When you want to get better at hill walking, you certainly don’t start off with a long day in the Alps! With everything new for our bodies, you should start off by laying better and more solid foundations so that your body adapts to its ‘new’ needs. The better your ‘foundations’, the more adaptable and protective your body is for the stresses and strains that we place on it.
I suspect if Carol had started off by adding in an hour of standing and then sitting for an hour and gradually adding in a bit more, she would have felt better. This may need to happen over the course of a few weeks.
In my opinion, I don’t think standing desks are for people to stand all day. I think it is a much better approach to do some sitting and some standing and mix it about. Doing it this way, you may stand for 3, 4 or 5 hours over the day in total. Your body gets to experience both.
I also get patients to stand with their feet in different positions to add variability. It encourages you to move more and this undoubtedly IS good for you.
If you have any muscle or joint problems or would like to come and see one of our Osteopaths, call 020 8605 2323.
Blog post by James Dodd

3 tips for Knee Rehabilitation and the need to be patient!
My Knee Rehabilitation! Nothing much to write today, other than I have been gradually increasing the amount of walking I have been doing and very clearly, it was too much! My knee was feeling unstable and it was ‘talking’ to me more. It was not unstable in any way. But it was just telling me to back off and I needed to listen. Knee rehabilitation after surgery takes time!

My Knee Rehabilitation! Nothing much to write today, other than I have been gradually increasing the amount of walking I have been doing and very clearly, it was too much! My knee was feeling unstable and it was ‘talking’ to me more. It was not unstable in any way. But it was just telling me to back off and I needed to listen. Knee rehabilitation after surgery takes time!
At only just over 2 weeks post operatively, mild swelling and inflammation was still present and the areas that had been cut inside were still sensitive.
What I did note, was that there were other aggravating factors having an impact. My footwear and the terrain that I had been walking on.
My shoes have been harder underneath with little or no give; this would have created more ‘jarring’ through to my knee. We have been increasing the distance that was walked, this inevitably included more hills, both up and down. In Cornwall these can be steep, especially in some of the beautiful towns that we visited.
So what did I do? The patient backed off and walked less! I wore softer shoes with more give in the soles.
I STOPPED being stubborn and soldiering on! It is so easy to just say….”Let’s carry on, it will be fine.” Clearly, it was not!
But I kept on with the same exercises without adding any more and would resume with more as soon as I was able.
I kept on reminding myself. It was ONLY 17 days post surgery and I am good with that. Healing takes time!!
Those 3 tips I mentioned.
I have really found walking is great- it is ‘free’ and being outside is brilliant for you in so many other ways too. Integration of your exercises is really important. Trying to work your knee in an integrated way joins other joints and muscles together. Your knee never works by itself.! Don’t underestimate how important your foot is. Your knee is a bit of a slave to your foot and so a really well moving foot allows your knee to track and load with greater efficiency.
More soon.
As Osteopaths at Back to Back, we recognise that it is crucial for post surgical rehabilitation to be UNIQUE to THE INDIVIDUAL. Exercises should be given to YOU and for YOUR problem and for YOUR stage of healing. The progression of exercises is also unique to the patient and given under the advice of a good health practitioner.
The above is all the opinion of Back to Back.
If you are concerned in anyway about your rehab, do come in and see one of our highly trained team.
Blog by James Dodd